Telehealth is no longer an afterthought or a “COVID-era backup plan.” It’s now the digital front door of healthcare. In fact, 76% of U.S. hospitals now use some form of telemedicine, not just for convenience, but because patients expect it and payers are willing to reimburse it.
But here’s the catch: building a telehealth app isn’t just about adding a video feature and calling it a day. If you want something real, something that clinicians trust, patients actually use, and insurers pay for, you need more than just a pretty UI. You need workflows that think like a doctor, data security that satisfies compliance, and integrations that make care coordination seamless.
This guide doesn’t sugarcoat the journey or throw generic steps at you. It’s a practical breakdown of what it takes to build a serious telehealth app, the kind that doesn’t burn out after its first release or blow your budget before you get your first patient onboard.
Whether you’re looking to bring a telemedicine app development solution to market, scale remote care, or partner with a healthcare app development company that actually understands clinical nuances, you’re in the right place.
Let’s get into the real details of what makes a telehealth app work in present times.
Telehealth Isn’t Optional Anymore. Here’s the Data That Proves It
Before we talk code, features, or compliance, let’s get on the same page about what’s happening in healthcare right now. Telehealth isn’t a backup plan for emergencies or a “pandemic-era trend” anymore, it has cemented itself as a core layer of care delivery.
Here’s the reality backed by the numbers that matter:
The U.S. telehealth market is already worth ~$50 billion and growing fast
Remote Patient Monitoring (RPM) is no longer niche, 81% of clinicians now use RPM, up more than 300% since 2021
Telehealth isn’t a temporary strategy, most U.S. hospitals still incorporate it as part of long-term care delivery
Convenience is a dealbreaker: 1 in 4 consumers say they’d switch providers if virtual care isn’t an option
Satisfaction is high, patients who use telehealth consistently rate the experience positively
Telehealth reduces missed appointments, virtual visits often outperform in-person care in completion rates
CMS now reimburses 80+ telehealth-eligible services, with updated flexibility around audio-only care
Smart virtual care workflows have been associated with reduced clinician burnout, especially around documentation and repetitive admin tasks
What this means for health tech teams and care providers:
Telehealth is now table stakes. It’s no longer about "launching a virtual care app," it’s about building something that works with clinical workflows, satisfies payer rules, protects patient data, and actually solves a care access problem.
That’s why building a telehealth app today goes way beyond adding a login button and a video chat SDK. It's about architecting care, not just coding features.
Ready to dive deeper? Let’s talk about what a working telehealth app really needs next.
What Telehealth Apps Actually Need to Work (Beyond Video Calls)
Let’s get this straight, a telehealth app isn’t “just another software project.” It’s a care delivery platform. And if you treat it like a chat app with a stethoscope emoji, you’ll end up rebuilding it six months later when clinicians reject it, patients drop off, or payers refuse to cover it.
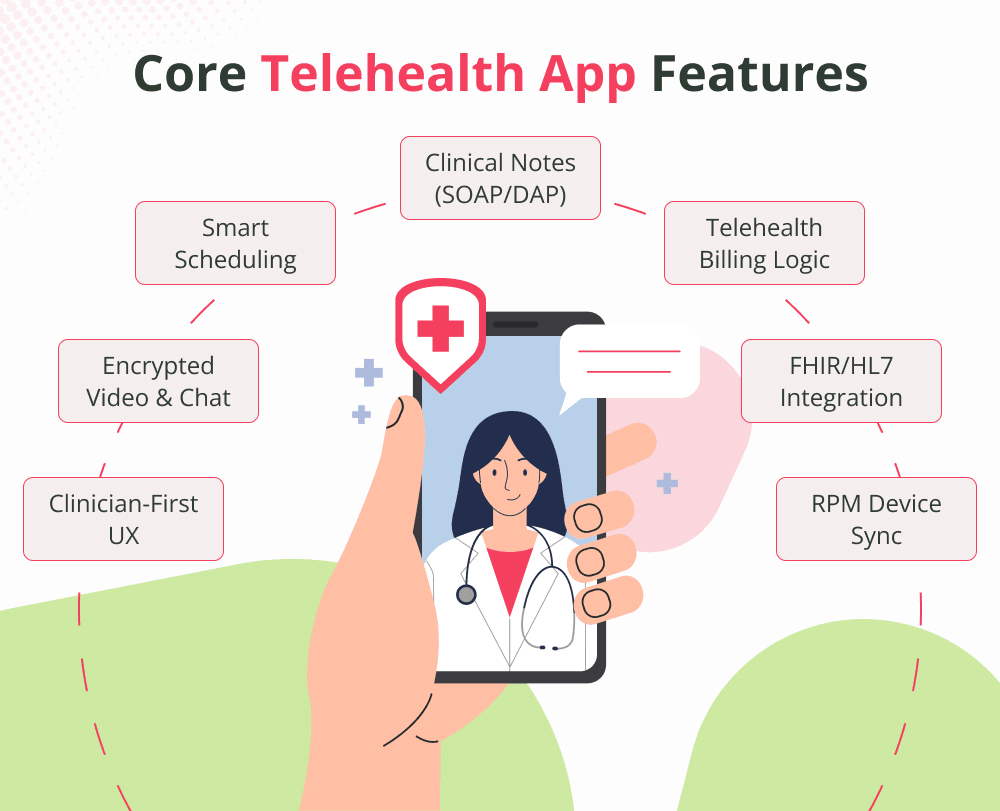
A clinical-grade telehealth platform needs to be built around real-world healthcare workflows. It must support:
The Entire Visit Lifecycle
From appointment booking → clinical documentation → billing → follow-up notes. And all of it needs to flow seamlessly between patients, providers, and systems.
That means:
Scheduling that auto-syncs with provider calendars
Intelligent reminders for patients (with time zone handling)
Easy rescheduling and cancellation pathways
Built-in prep workflows (Complete intake form before visit)
HIPAA-Proof Communication
Every message, document, or live session must:
Be encrypted end-to-end
Comply with PHI storage rules
Log every interaction for audit purposes
Be role-aware (doctor, admin, patient, caregiver, etc.)
This isn’t optional and it’s why building “from scratch” without a compliance-first mindset is a liability.
Real-Time Clinical Documentation
Clinicians shouldn't have to use sticky notes or external systems while on a call. A good platform:
Lets them write SOAP or DAP notes during or after the session
Ties documentation to CPT or ICD codes for billing
Supports auto-logging and signature capture
Syncs to an EHR (or uses FHIR/HL7 if integration-ready)
Integrated Medical Data and Device Support
Telehealth isn’t just video. It's monitoring, tracking, and decision support. That means:
Labs, prescriptions, and care plans available in one place
Insurance-Ready Billing and Payer Logic
Telehealth needs to get paid. If billing isn’t part of the product logic, you're building a toy.
Support for 80+ CMS telehealth CPT codes
Consent and session logs for audit readiness
Built-in modifier logic (place of service, session type, etc.)
Integration with claims or RCM workflows
A UX Clinicians Actually Like (Critical for Adoption)
Doctors want tools that feel more like iOS, and less like 1998 hospital software. That means:
Clean, focused interface with minimal friction
Multi-device support: desktops in clinic, tablets at home
One-click access to past notes, meds, and anatomy
Bottom line: A working telehealth app isn’t “Add Video + Go Live.” It’s:
Build a complete visit experience that patients trust, clinicians adopt, and payers approve.
And if you want to avoid the years-long learning curve of building everything in-house? This is where partnering with a real healthcare app development company or a proven mobile app development company in USA becomes the difference between scaling or stalling.
What to Build First - Feature vs Function vs Compliance
Here’s the truth that nobody says out loud: it’s easy to overbuild a telehealth app and still miss what really matters in the first release. The fastest way to fail is to build for “wow” instead of building for workflow.
In healthcare, prioritization > planning. Your V1 doesn’t need to do everything, it needs to do the right things, safely and compliantly.
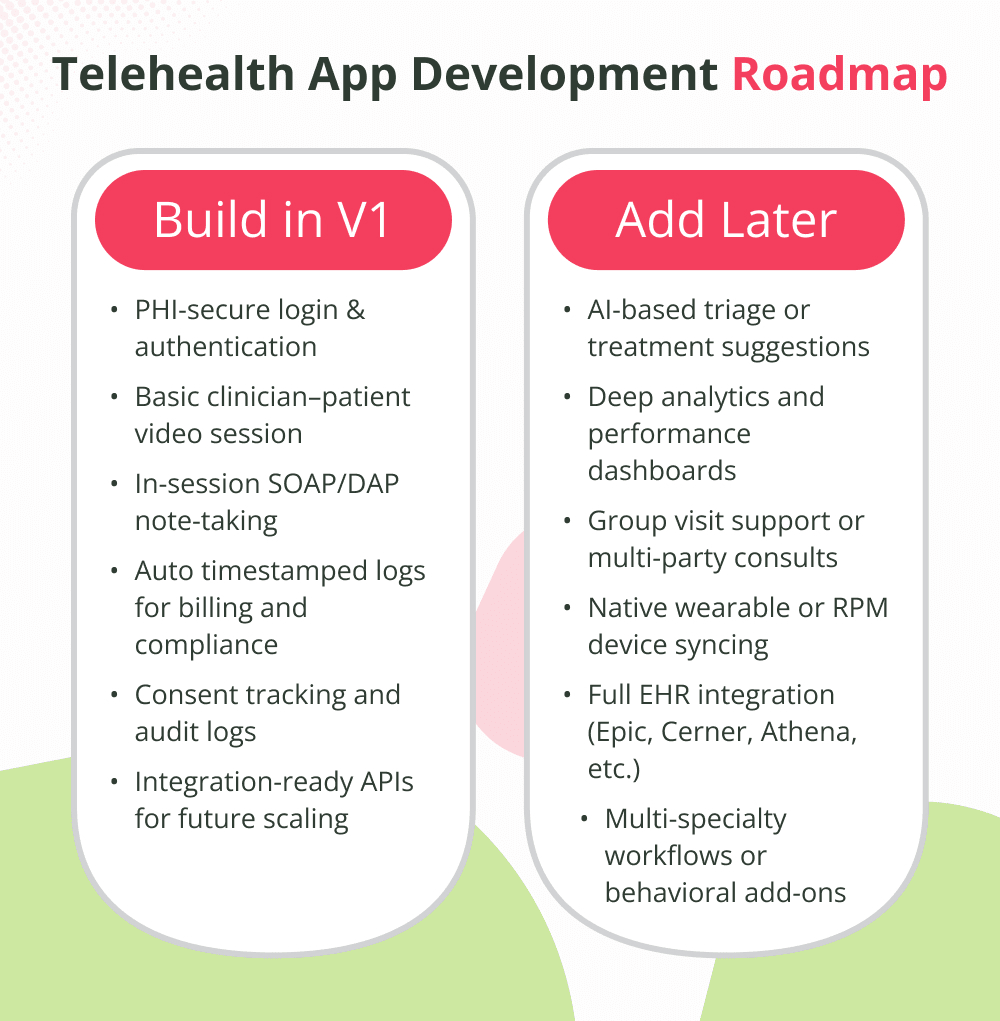
Start Here: The Core of a Real V1
If you're building your first version of a telemedicine platform, this is what your MVP actually needs:
PHI-secure authentication
Login, identity verification, and data protection compliant with HIPAA, no exceptions.
Simple, reliable video visits
A basic, high-quality clinician–patient video session, recording only where state or specialty rules allow.
Real-time clinical documentation
Let providers write SOAP notes during or after a call. Even better? Link those fields to CPT or ICD codes for billing downstream.
Built-in visit logging
Session timestamps and consent logs are non-negotiable. They’re how you bill, audit, and prove care happened.
Integration-ready APIs (even if you delay the integration)
You may not be ready to sync with EHRs like Epic or Cerner in V1 but your architecture should be ready when you are.
Skip (for now): The Stuff That Bloats Your Build
You don’t need these in your first release and trying to include them early can slow you down and burn your budget:
Fully automated AI-driven triage or recommendations
Chart insights and deep performance dashboards
Full wearable or RPM device sync unless you’re targeting chronic care from day one
Multi-specialty UX with configurable clinical flows
Group video sessions or interpreter layers
Native EHR integration before your user base even hits double digits
The Key Takeaway
V1 isn’t about shining, it’s about sticking. Keep the workflow small, proven, and safe.
Build Version 1 for one user persona, one clinical use case, one repeatable workflow… and build it well.
If you're working with a healthcare app development company that understands compliance and clinical flows, they’ll push you toward what gets clinical trust and payer approval first and let the bells and whistles wait their turn.
Telehealth App Development Roadmap: What to Build First vs What to Layer in Later
A practical guide for founders, healthcare leaders, and product teams prioritizing version 1.0 without sacrificing scale, safety, or reimbursement.
The Hybrid Build vs Buy Approach: How Smart Telehealth Apps Launch 3× Faster (Without Cutting Corners)
Here’s a myth that stalls more telehealth products than regulation ever has:
“We need to build everything from scratch if we want it to be secure, scalable, and clinical-grade.”
Reality? That’s the most expensive way to build and almost always the slowest.
The most successful health tech teams don’t “build it all.” They assemble the parts that should already exist in the world (HIPAA video, patient messaging, PHI-safe cloud storage), and custom-build only what truly differentiates their product like clinical workflows, specialty-specific UX, or proprietary care logic.
That’s the hybrid build-vs-buy approach. And in telehealth, it’s not a trend. It’s survival.
Why “Fully Custom” Doesn’t Work in Healthcare
If you’re building a healthcare app that handles PHI, video consults, or electronic prescriptions, a purely custom build means:
Longer time to market (think 12–18 months just for the basics)
Higher upfront cost (compliance alone raises the bill)
Increased legal and security risk
Rebuilding features others have already perfected like secure chat or consent logging
By the time you're done, another app will already be eating your market.
So What Should Be Custom-Built?
These are the areas you do want to fully own because they’re what define your product’s clinical and business value:
Your care model workflow (e.g., rehab vs psychiatry vs chronic disease)
Your user interface for patients and clinicians
Treatment note structure, documentation flow, or specialty logic
Outcomes tracking, goal dashboards, or personalized patient plans
This is your IP. This is where clinical trust, retention, and differentiation happen.
And What Should Be Bought or Integrated?
These components already exist as HIPAA-ready SDKs or enterprise-grade APIs and there’s no benefit in reinventing them from scratch.
If a vendor can give you a compliant, proven component in days instead of months, you don’t code it, you plug it in.
Pro Tip: Map Workflows Before Writing Code
Here's how smart teams decide what to build vs buy:
Define the provider and patient journeys in detail
Circle the steps that make your solution unique
Circle the steps that make your solution unique
Everything else? Automate, integrate, outsource, or license
Hybrid is smarter, cheaper, and safer especially in healthcare, where the cost of getting it wrong isn’t just downtime. It’s liability.
In short:
Don’t build everything. Build what matters.
And if this isn’t your first regulated product? You already know the partner you choose, whether a plug-in API, a health cloud, or a healthcare app development company will either speed you up or slow you way down.
The Real Cost of Telehealth App Development (And What’s Worth Paying For)
One of the biggest misconceptions in health tech is that “building an app” is the same as “building a telehealth platform.” In reality, the cost of a telehealth app isn’t driven by how many screens it has, it’s driven by what kind of healthcare delivery system you’re enabling, and what regulations you're bound by.
So if you're budgeting for a telehealth product, here’s what you need to know:
What Drives the Cost of a Telehealth App?
Scope and Complexity of Clinical Workflows
Are you supporting primary care consults? Behavioral health? Multi-specialty group visits? Chronic care with device syncing?
Each layer adds new workflows, testing scenarios, integrations, and user types.
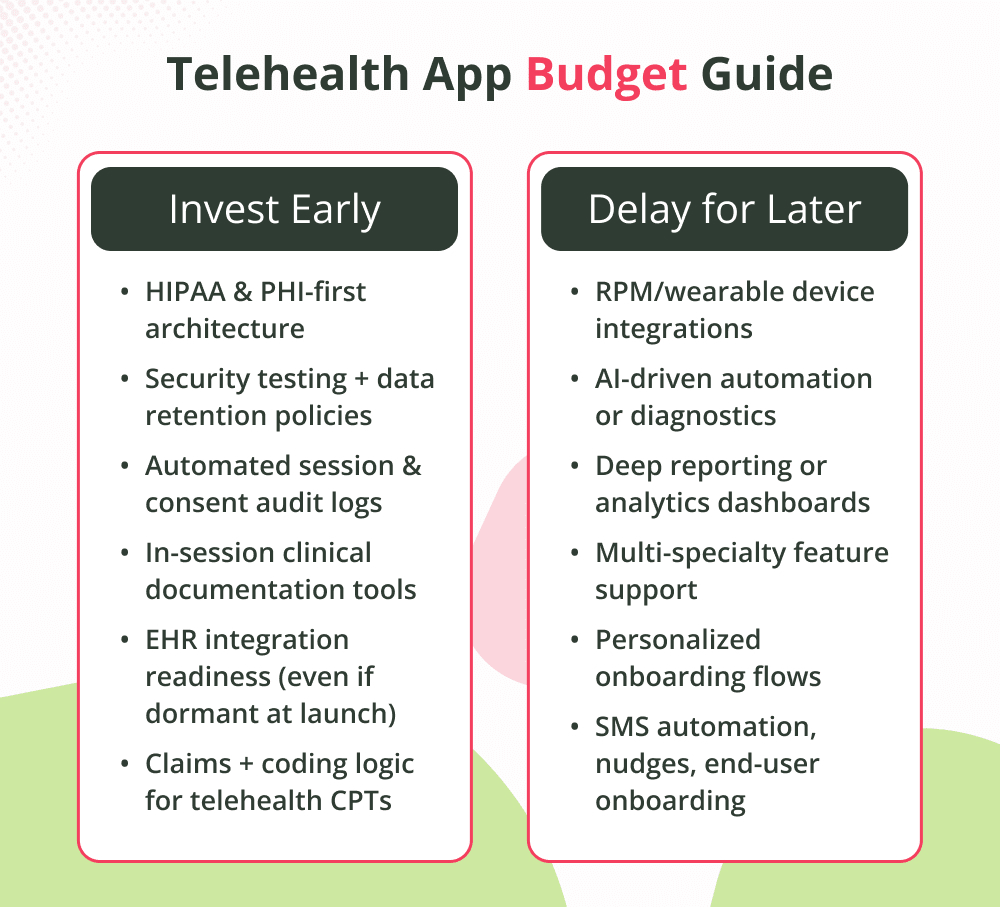
Compliance and Security Infrastructure
HIPAA isn’t a one-time checkbox, it’s an ongoing system requirement.
Budget for:
Encryption (in transit & at rest)
PHI-safe databases (not just a “cloud server”)
Logging, consent, and identity checks
Legal/BAA alignment
That’s why a healthcare app development company with built-in HIPAA expertise often becomes a cost saver, not a line item.
EHR, RPM, and Third-Party Integrations
Integrating with Epic, Cerner, athena, or Redox isn’t cheap but it’s necessary if you're building for healthcare organizations. Same with device data (glucose monitors, wearables, etc.).
Payer and Billing Logic
Submitting claims, separating private pay vs insurance, adding telehealth modifiers, and tracking time-stamped logs, all of this requires engineering + RCM expertise, plus ongoing updates based on CMS rules.
Regulated Features (E.g., eRx, asynchronous consults)
Telehealth App Budget Guide: What to Invest in Early vs What to Delay
Hidden Pitfalls in Telemedicine Integrations
Integrations are where most telehealth apps break, not during launch, but in year two, when the clinical team starts scaling and the tech debt starts biting.
Here’s what teams consistently underestimate:
The EHR “Plug-and-Play” Myth
FHIR/HL7 doesn’t mean friction-free. Every EHR behaves differently, access is restricted, and data mappings are often inconsistent.
Integration ≠ interoperability, especially in healthcare.
RPM Data Chaos
Device data isn’t standardized, not by unit, timestamp, or format.
What starts as “just sync vitals” becomes “let’s decode 200 different ways to send blood pressure.”
States Have Their Own Rules
Billing codes, eRx workflows, even video laws vary by state. Build once → maintain forever.
Video Isn’t Cosmetic, It’s Clinical
Laggy or low-res consults don’t just frustrate doctors. They break trust and interrupt assessments like speech, facial movement, or rash severity.
✅ Integration Survival Tip
Go slow. Test in the hands of clinicians. Fix with real feedback, not in staging.
Where AI Fits (Today, Not Tomorrow) in Telehealth
AI is already reshaping telehealth but not where most people think. You don’t need “robot doctors” or diagnosing chatbots to get real value. Today’s best uses of AI in virtual care are assistive, not autonomous.
Here’s what’s working now:
Ambient Clinical Documentation
Transforms live or recorded consults into structured SOAP notes, saving providers an hour a day.
Not replacing doctors, just replacing typing.
Smart Coding & Billing Support
Suggests CPT codes based on notes and visit type. Fewer denials. Faster payer cycles.
AI-Assisted Triage
Guides patients to the right visit type (chat, video, in-person) without guesswork. Cuts down no-show or wrong-setting consults.
Outcome Pattern Insights
Tracks patient metrics to alert clinicians if vitals or trends signal risk only after human validation.
How to Choose the Right Healthcare App Development Company (Fast Checklist)
Most dev shops can build an app. Very few can build a telehealth product that meets clinical, legal, and payer expectations. Here’s how to tell the difference, fast:
Ask These 5 Questions
Do you build HIPAA in from Day 1 or bolt it on later?
If they say “we’ll add it later,” walk away.
Can I see a live telehealth app you're already powering?
If they can’t show actual usage in clinics, they haven't done it.
Do you own FHIR/HL7 experience or outsource integration?
Outsourced handling means slower timelines and compliance risk.
What’s your uptime plan and PHI recovery policy?
If they don’t mention encryption, redundancy, or BAA responsibility, they’re not ready.
Can you legally deliver as a U.S.-compliant mobile app development company?
Because offshore + PHI = liability (and fines).
Red Flags?
“We can use any cloud”
“Compliance isn’t needed for MVP!”
“Yeah, Zoom is enough”
“We’ve never handled CPT codes or claims before”
If it sounds like they don’t understand auditors, clinicians, or payers, they don’t.
What the Right Partner Sounds Like
“We start with HIPAA data models.”
“We support FHIR v4 with fallbacks.”
“Here’s our downtime + recovery policy.”
“Here’s a telehealth app we launched in 6 months that's still scaling.”
Anything less? Keep looking.
Telehealth Is Changing Care And You Can Shape It
Telehealth isn’t just another digital channel, it's becoming a core part of how people access medicine, connect with providers, and manage long-term health.
When telehealth is built thoughtfully with workflows that feel natural for clinicians, UX that feels calming for patients, and systems that stand up to compliance and payor pressure, it becomes more than a product.
It becomes a priority in care delivery.
That’s why choosing the right healthcare app development company isn’t a technical decision, it’s a care decision. And the future belongs to the teams who design telehealth like care matters more than
Code.
🎧 Podcast: How to Build a Modern Telehealth App That Lasts
Tune in to explore the tech, features, and compliance secrets behind scalable telemedicine apps.
Get practical insights from real healthcare app development experts with no fluff—just what works.
Ready to Build Telehealth That Works in the Real World?
If you're serious about creating a telehealth platform that clinicians trust and patients actually use, we’re ready to help.
Talk to the team that builds more than apps.
We build care experiences at scale.
Prithi is currently working as Android Architect at VT Netzwelt. He is having 12+ years of industry experience. Prithi has worked on different technology stacks including Android, Kotlin, iOS, Java, J2EE, React Native, Flutter, Web Services. Prithi is currently exploring AI and ML in Mobile app development.
Swift vs React Native in 2026: compare performance, Apple features, security, maintenance, cost, and use cases to choose the right framework for your app.